Reproductive System Diseases
Cervical Cancer
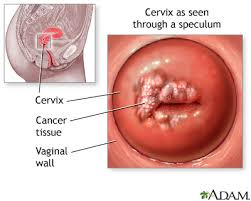
Cervical cancer starts in the cells of the cervix. The cervix is the narrow, lower part of the uterus (or womb). It is the passageway that connects the uterus to the vagina.
The cervix is part of a woman’s reproductive system. It makes mucus that helps sperm move from the vagina into the uterus or keeps sperm from entering the uterus. Every month during your menstrual period blood flows from the uterus through the cervix into the vagina. During pregnancy, the cervix is closed to keep the baby inside the uterus. During childbirth, the cervix opens (dilates) so that the baby can pass through the vagina.
Before cervical cancer develops, the cells of the cervix start to change and become abnormal. These abnormal cells are precancerous, meaning that they are not cancer. Precancerous changes to the cervix are called dysplasia of the cervix (or cervical dysplasia).
Dysplasia of the cervix is not cancer. It is a common precancerous change that can develop into cancer if it isn’t treated. It is important to know that most women with dysplasia do not develop cancer
Cervical cancer starts in the cells of the cervix. The cervix is the narrow, lower part of the uterus (or womb). It is the passageway that connects the uterus to the vagina.
The cervix is part of a woman’s reproductive system. It makes mucus that helps sperm move from the vagina into the uterus or keeps sperm from entering the uterus. Every month during your menstrual period blood flows from the uterus through the cervix into the vagina. During pregnancy, the cervix is closed to keep the baby inside the uterus. During childbirth, the cervix opens (dilates) so that the baby can pass through the vagina.
Before cervical cancer develops, the cells of the cervix start to change and become abnormal. These abnormal cells are precancerous, meaning that they are not cancer. Precancerous changes to the cervix are called dysplasia of the cervix (or cervical dysplasia).
Dysplasia of the cervix is not cancer. It is a common precancerous change that can develop into cancer if it isn’t treated. It is important to know that most women with dysplasia do not develop cancer
Breast Cancer
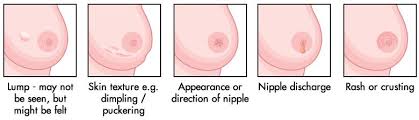
Breast cancer starts in the cells of the breast. The breast tissue covers an area larger than just the breast. It extends up to the collarbone and from the armpit across to the breastbone in the centre of the chest. The breasts sit on the chest muscles that cover the ribs. Each breast is made of glands, ducts (thin tubes) and fatty tissue. Lobules are groups of glands that can produce milk. Milk flows from the lobules through a network of ducts to the nipple. The nipple is in the centre of a darker area of skin called the areola. Fatty tissue fills the spaces between the lobules and ducts and protects them.
A woman’s breasts may feel different at different times of her menstrual cycle, sometimes becoming lumpy just before her period. Breast tissue also changes with age. Breast tissue in younger women is mostly made of glands and milk ducts, but older women’s breasts are made up mostly of fatty tissue.
The breasts also contain lymph vessels and lymph nodes, which are part of the lymphatic system. The lymphatic system helps fight infections. Lymph vessels move lymph fluid to the lymph nodes. Lymph nodes trap bacteria, cancer cells and other harmful substances. There are groups of lymph nodes near the breast under the arm, near the collarbone and in the chest behind the breastbone.
Cancer cells may start within the ducts (this is called ductal carcinoma) or in the lobules (lobular carcinoma). Ductal carcinoma is the most common type of breast cancer.
Prostate Cancer
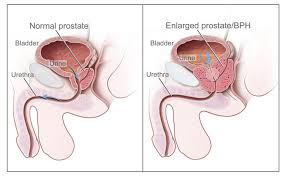
Prostate cancer starts in the cells of the prostate gland. The prostate is part of the male reproductive system. Its main function is to make part of the liquid (seminal fluid) that mixes with sperm from the testicles to make semen. Semen is ejaculated during sex.
The prostate is about the size of a large walnut. It is located close to the rectum just below the bladder at the base of the penis. The prostate surrounds the urethra, the tube that carries urine and semen through the penis.
Prostate cancer is the most common cancer in Canadian men. It usually grows slowly and can often be cured or managed successfully if caught early by regular annual examination.
Impotence
Impotence is a common problem among men characterized by the consistent inability to sustain an erection sufficient for sexual intercourse or the inability to achieve ejaculation, or both. Impotence can vary. It can involve a total inability to achieve an erection or ejaculation, an inconsistent ability to do so, or a tendency to sustain only very brief erections.
The risk of impotence increases with age. It is four-fold higher in men in their 60s compared with those in their 40s according to a study published in the Journal of Urology (2000;163:460-463). Men with less education are also more likely to experience impotence, perhaps because they tend to have less healthy lifestyles, eat a less healthy diet, drink more and exercise less. Physical exercise tends to lessen the risk of impotence.
I'm sure that you have seen pharmaceutical advertising in doctor's offices on everything from tissues to note pads.
Well, in my book, this one should get the prize....

|

|
|
Gonorrhea
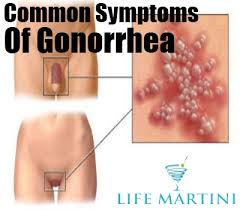
is a sexually transmitted disease (STD). Gonorrhea is caused by Neisseria gonorrhoeae, a bacterium that can grow and multiply easily in the warm, moist areas of the reproductive tract, including the cervix (opening to the womb), uterus (womb), and fallopian tubes (egg canals) in women, and in the urethra (urine canal) in women and men. The bacterium can also grow in the mouth, throat, eyes, and anus. Gonorrhea is a very common infectious disease. CDC estimates that more than 700,000 persons in the U.S. get new gonorrheal infections each year. Only about half of these infections are reported to CDC. In 2006, 358,366 cases of gonorrhea were reported to CDC. In the period from 1975 to 1997, the national gonorrhea rate declined, following the implementation of the national gonorrhea control program in the mid-1970s. After several years of stable gonorrhea rates, however, the national gonorrhea rate increased for the second consecutive year. In 2006, the rate of reported gonorrheal infections was 120.9 per 100,000 persons. Gonorrhea is spread through contact with the penis, vagina, mouth, or anus. Ejaculation does not have to occur for gonorrhea to be transmitted or acquired. Gonorrhea can also be spread from mother to baby during delivery. People who have had gonorrhea and received treatment may get infected again if they have sexual contact with a person infected with gonorrhea. Some men with gonorrhea may have no symptoms at all. However, some men have signs or symptoms that appear two to five days after infection; symptoms can take as long as 30 days to appear. Symptoms and signs include a burning sensation when urinating, or a white, yellow, or green discharge from the penis. Sometimes men with gonorrhea get painful or swollen testicles. In women, the symptoms of gonorrhea are often mild, but most women who are infected have no symptoms. Even when a woman has symptoms, they can be so non-specific as to be mistaken for a bladder or vaginal infection. The initial symptoms and signs in women include a painful or burning sensation when urinating, increased vaginal discharge, or vaginal bleeding between periods. Women with gonorrhea are at risk of developing serious complications from the infection, regardless of the presence or severity of symptoms. 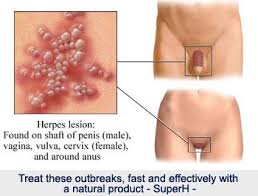
|
|
Herpes simplex II
HSV is a large, double stranded DNA virus. All the programming of the virus’ ability to infect someone is contained in the DNA. The DNA is packaged in a “diamond like” protein structure, called an icosahedron. The virus also has an “over coat”, the envelope, which is necessary for the “docking” procedure when the virus infects a cell. In other words, an HSV particle without the envelope is not infectious, since it cannot enter the cell.
The virus gains entry into the body, not through intact skin, but through mucous membranes, such as the oral region, vagina, tip of the penis, or the eye. The virus will first replicate (make copies of itself) inside surface cells at these sites, eventually killing the infected surface cells. In a person with normal immunity, the immune system is quickly mobilized to contain the primary infection.
However, before this happens, the virus gains entry to the nerve cell end-plates (structures that help us to feel things like pain and temperature), present at the skin surface. The end-plates connect to the more deeply located nerve cell body through an elongated nerve fibre or axon. This cell in turn is connected to “serially coupled” layers of internal nerve cells, which eventually lead to a ganglion, which is a collection of nerve cell bodies just like a node in an electricity grid. Through such intricate connections the nerve cells eventually lead into and communicate with the central nervous system or the brain. The axons are protected by “myelin blankets”, just like the insulating material around electrical wires, but the endings are bare, as are the nodes where one nerve cell extension connects with the next (synapse). It is thought that the virus sheds its envelope as soon as it has entered the nerve and uses the axon as a conduit, hiding from immune system attack, as if it were inside a “Trojan Horse”.
HSV has specifically chosen the nerve cell body and ultimately the ganglion (HSV-1 resides in the trigeminal ganglion; HSV-2 resides in the sacral ganglia) as a site where it remains dormant. It is from these locations that the virus may reactivate from its dormant state to the respective innervated (nerve-cell-serviced) body areas. This is why dormant virus from the trigeminal ganglion (oral or facial area) reactivates in the oral or facial region, whereas the dormant virus from the sacral ganglion (lower back/spine area) reactivate to the genital area or the buttock.
Within a day of infection, the naked virus (nucleocapsid) arrives at the nerve cell nucleus, and it “injects” its genetic material (DNA).It then resides in the nerve cell nucleus in a dormant (latent) form.
According to most researchers, virus replication will not occur at this stage and no new virus particles will be formedThe precise molecular mechanisms for this event (establishment and maintenance of latency) are unknown, but appear to reflect an interplay between viral and nerve cell factors.
However, other researchers argue that a low level of replication must occur in order to keep the virus machine “well oiled”. This could be compared to car maintenance. For proper functioning, it is not a good idea to leave a car in the garage for years, but to drive it at least occasionally. If this were the case for HSV, it would likely result in low level viral shedding at the peripheral skin site.
It is important, from the virus “survival” point of view, to be able to “fire up” and begin to replicate should circumstances become uncomfortable inside the neuron (i.e. the infected person suffers a trauma, acquires a severe disease, becomes immunocompromised, or dies).
We do not understand why stress and sunshine, for example, tend to trigger HSV reactivation. When this happens, new virus particles are created and transported back to the skin and mucous membranes through the neuronal highway. They then begin to replicate in the surface cells, creating a blister in the form of a cold sore or genital herpes. The surface cells balloon up and become filled with fluid. This fluid contains millions of infectious viral particles.
We believe that the infected nerve cells usually survive during this reactivation process. We also think that HSV particles not only travel down to the skin and mucous membranes, but may also travel in the opposite direction leading them closer to the brain. Some researchers suggest that healthy immunocompetent people may, in fact, harbor dormant virus inside the brain.
HSV spreads from person to person by direct contact with infected secretions, such as through kissing or sexual intercourse.
HSV is a large, double stranded DNA virus. All the programming of the virus’ ability to infect someone is contained in the DNA. The DNA is packaged in a “diamond like” protein structure, called an icosahedron. The virus also has an “over coat”, the envelope, which is necessary for the “docking” procedure when the virus infects a cell. In other words, an HSV particle without the envelope is not infectious, since it cannot enter the cell.
The virus gains entry into the body, not through intact skin, but through mucous membranes, such as the oral region, vagina, tip of the penis, or the eye. The virus will first replicate (make copies of itself) inside surface cells at these sites, eventually killing the infected surface cells. In a person with normal immunity, the immune system is quickly mobilized to contain the primary infection.
However, before this happens, the virus gains entry to the nerve cell end-plates (structures that help us to feel things like pain and temperature), present at the skin surface. The end-plates connect to the more deeply located nerve cell body through an elongated nerve fibre or axon. This cell in turn is connected to “serially coupled” layers of internal nerve cells, which eventually lead to a ganglion, which is a collection of nerve cell bodies just like a node in an electricity grid. Through such intricate connections the nerve cells eventually lead into and communicate with the central nervous system or the brain. The axons are protected by “myelin blankets”, just like the insulating material around electrical wires, but the endings are bare, as are the nodes where one nerve cell extension connects with the next (synapse). It is thought that the virus sheds its envelope as soon as it has entered the nerve and uses the axon as a conduit, hiding from immune system attack, as if it were inside a “Trojan Horse”.
HSV has specifically chosen the nerve cell body and ultimately the ganglion (HSV-1 resides in the trigeminal ganglion; HSV-2 resides in the sacral ganglia) as a site where it remains dormant. It is from these locations that the virus may reactivate from its dormant state to the respective innervated (nerve-cell-serviced) body areas. This is why dormant virus from the trigeminal ganglion (oral or facial area) reactivates in the oral or facial region, whereas the dormant virus from the sacral ganglion (lower back/spine area) reactivate to the genital area or the buttock.
Within a day of infection, the naked virus (nucleocapsid) arrives at the nerve cell nucleus, and it “injects” its genetic material (DNA).It then resides in the nerve cell nucleus in a dormant (latent) form.
According to most researchers, virus replication will not occur at this stage and no new virus particles will be formedThe precise molecular mechanisms for this event (establishment and maintenance of latency) are unknown, but appear to reflect an interplay between viral and nerve cell factors.
However, other researchers argue that a low level of replication must occur in order to keep the virus machine “well oiled”. This could be compared to car maintenance. For proper functioning, it is not a good idea to leave a car in the garage for years, but to drive it at least occasionally. If this were the case for HSV, it would likely result in low level viral shedding at the peripheral skin site.
It is important, from the virus “survival” point of view, to be able to “fire up” and begin to replicate should circumstances become uncomfortable inside the neuron (i.e. the infected person suffers a trauma, acquires a severe disease, becomes immunocompromised, or dies).
We do not understand why stress and sunshine, for example, tend to trigger HSV reactivation. When this happens, new virus particles are created and transported back to the skin and mucous membranes through the neuronal highway. They then begin to replicate in the surface cells, creating a blister in the form of a cold sore or genital herpes. The surface cells balloon up and become filled with fluid. This fluid contains millions of infectious viral particles.
We believe that the infected nerve cells usually survive during this reactivation process. We also think that HSV particles not only travel down to the skin and mucous membranes, but may also travel in the opposite direction leading them closer to the brain. Some researchers suggest that healthy immunocompetent people may, in fact, harbor dormant virus inside the brain.
HSV spreads from person to person by direct contact with infected secretions, such as through kissing or sexual intercourse.
Syphilis
Syphilis is a sexually transmitted disease (STD) caused by the bacterium Treponema pallidum. It has often been called “the great imitator” because so many of the signs and symptoms are indistinguishable from those of other diseases.
In the United States, health officials reported over 36,000 cases of syphilis in 2006, including 9,756 cases of primary and secondary (P&S) syphilis. In 2006, half of all P&S syphilis cases were reported from 20 counties and 2 cities; and most P&S syphilis cases occurred in persons 20 to 39 years of age. The incidence of P&S syphilis was highest in women 20 to 24 years of age and in men 35 to 39 years of age. Reported cases of congenital syphilis in newborns increased from 2005 to 2006, with 339 new cases reported in 2005 compared to 349 cases in 2006.
Between 2005 and 2006, the number of reported P&S syphilis cases increased 11.8 percent. P&S rates have increased in males each year between 2000 and 2006 from 2.6 to 5.7 and among females between 2004 and 2006. In 2006, 64% of the reported P&S syphilis cases were among men who have sex with men (MSM).
Syphilis is passed from person to person through direct contact with a syphilis sore. Sores occur mainly on the external genitals, vagina, anus, or in the rectum. Sores also can occur on the lips and in the mouth. Transmission of the organism occurs during vaginal, anal, or oral sex. Pregnant women with the disease can pass it to the babies they are carrying. Syphilis cannot be spread through contact with toilet seats, doorknobs, swimming pools, hot tubs, bathtubs, shared clothing, or eating utensils.
Many people infected with syphilis do not have any symptoms for years, yet remain at risk for late complications if they are not treated. Although transmission occurs from persons with sores who are in the primary or secondary stage, many of these sores are unrecognized. Thus, transmission may occur from persons who are unaware of their infection.
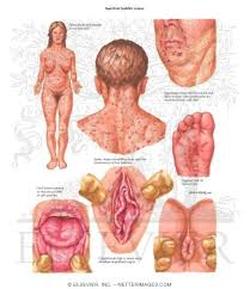
The primary stage of syphilis is usually marked by the appearance of a single sore (called a chancre), but there may be multiple sores. The time between infection with syphilis and the start of the first symptom can range from 10 to 90 days (average 21 days). The chancre is usually firm, round, small, and painless. It appears at the spot where syphilis entered the body. The chancre lasts 3 to 6 weeks, and it heals without treatment. However, if adequate treatment is not administered, the infection progresses to the secondary stage.
Skin rash and mucous membrane lesions characterize the secondary stage. This stage typically starts with the development of a rash on one or more areas of the body. The rash usually does not cause itching. Rashes associated with secondary syphilis can appear as the chancre is healing or several weeks after the chancre has healed. The characteristic rash of secondary syphilis may appear as rough, red, or reddish brown spots both on the palms of the hands and the bottoms of the feet. However, rashes with a different appearance may occur on other parts of the body, sometimes resembling rashes caused by other diseases. Sometimes rashes associated with secondary syphilis are so faint that they are not noticed. In addition to rashes, symptoms of secondary syphilis may include fever, swollen lymph glands, sore throat, patchy hair loss, headaches, weight loss, muscle aches, and fatigue. The signs and symptoms of secondary syphilis will resolve with or without treatment, but without treatment, the infection will progress to the latent and possibly late stages of disease.
The latent (hidden) stage of syphilis begins when primary and secondary symptoms disappear. Without treatment, the infected person will continue to have syphilis even though there are no signs or symptoms; infection remains in the body. This latent stage can last for years. The late stages of syphilis can develop in about 15% of people who have not been treated for syphilis, and can appear 10 – 20 years after infection was first acquired. In the late stages of syphilis, the disease may subsequently damage the internal organs, including the brain, nerves, eyes, heart, blood vessels, liver, bones, and joints. Signs and symptoms of the late stage of syphilis include difficulty coordinating muscle movements, paralysis, numbness, gradual blindness, and dementia. This damage may be serious enough to cause death.
The syphilis bacterium can infect the baby of a woman during her pregnancy. Depending on how long a pregnant woman has been infected, she may have a high risk of having a stillbirth (a baby born dead) or of giving birth to a baby who dies shortly after birth. An infected baby may be born without signs or symptoms of disease. However, if not treated immediately, the baby may develop serious problems within a few weeks. Untreated babies may become developmentally delayed, have seizures, or die.
Some health care providers can diagnose syphilis by examining material from a chancre (infectious sore) using a special microscope called a dark-field microscope. If syphilis bacteria are present in the sore, they will show up when observed through the microscope.
A blood test is another way to determine whether someone has syphilis. Shortly after infection occurs, the body produces syphilis antibodies that can be detected by an accurate, safe, and inexpensive blood test. A low level of antibodies will likely stay in the blood for months or years even after the disease has been successfully treated. Because untreated syphilis in a pregnant woman can infect and possibly kill her developing baby, every pregnant woman should have a blood test for syphilis.
Genital sores (chancres) caused by syphilis make it easier to transmit and acquire HIV infection sexually. There is an estimated 2- to 5-fold increased risk of acquiring HIV if exposed to that infection when syphilis is present.
Ulcerative STDs that cause sores, ulcers, or breaks in the skin or mucous membranes, such as syphilis, disrupt barriers that provide protection against infections. The genital ulcers caused by syphilis can bleed easily, and when they come into contact with oral and rectal mucosa during sex, increase the infectiousness of and susceptibility to HIV. Having other STDs is also an important predictor for becoming HIV infected because STDs are a marker for behaviors associated with HIV transmission.
Syphilis is easy to cure in its early stages. A single intramuscular injection of penicillin, an antibiotic, will cure a person who has had syphilis for less than a year. Additional doses are needed to treat someone who has had syphilis for longer than a year. For people who are allergic to penicillin, other antibiotics are available to treat syphilis. There are no home remedies or over-the-counter drugs that will cure syphilis. Treatment will kill the syphilis bacterium and prevent further damage, but it will not repair damage already done.
Because effective treatment is available, it is important that persons be screened for syphilis on an on-going basis if their sexual behaviors put them at risk for STDs.
Persons who receive syphilis treatment must abstain from sexual contact with new partners until the syphilis sores are completely healed. Persons with syphilis must notify their sex partners so that they also can be tested and receive treatment if necessary.
Syphilis is a sexually transmitted disease (STD) caused by the bacterium Treponema pallidum. It has often been called “the great imitator” because so many of the signs and symptoms are indistinguishable from those of other diseases.
In the United States, health officials reported over 36,000 cases of syphilis in 2006, including 9,756 cases of primary and secondary (P&S) syphilis. In 2006, half of all P&S syphilis cases were reported from 20 counties and 2 cities; and most P&S syphilis cases occurred in persons 20 to 39 years of age. The incidence of P&S syphilis was highest in women 20 to 24 years of age and in men 35 to 39 years of age. Reported cases of congenital syphilis in newborns increased from 2005 to 2006, with 339 new cases reported in 2005 compared to 349 cases in 2006.
Between 2005 and 2006, the number of reported P&S syphilis cases increased 11.8 percent. P&S rates have increased in males each year between 2000 and 2006 from 2.6 to 5.7 and among females between 2004 and 2006. In 2006, 64% of the reported P&S syphilis cases were among men who have sex with men (MSM).
Syphilis is passed from person to person through direct contact with a syphilis sore. Sores occur mainly on the external genitals, vagina, anus, or in the rectum. Sores also can occur on the lips and in the mouth. Transmission of the organism occurs during vaginal, anal, or oral sex. Pregnant women with the disease can pass it to the babies they are carrying. Syphilis cannot be spread through contact with toilet seats, doorknobs, swimming pools, hot tubs, bathtubs, shared clothing, or eating utensils.
Many people infected with syphilis do not have any symptoms for years, yet remain at risk for late complications if they are not treated. Although transmission occurs from persons with sores who are in the primary or secondary stage, many of these sores are unrecognized. Thus, transmission may occur from persons who are unaware of their infection.
The primary stage of syphilis is usually marked by the appearance of a single sore (called a chancre), but there may be multiple sores. The time between infection with syphilis and the start of the first symptom can range from 10 to 90 days (average 21 days). The chancre is usually firm, round, small, and painless. It appears at the spot where syphilis entered the body. The chancre lasts 3 to 6 weeks, and it heals without treatment. However, if adequate treatment is not administered, the infection progresses to the secondary stage.
Skin rash and mucous membrane lesions characterize the secondary stage. This stage typically starts with the development of a rash on one or more areas of the body. The rash usually does not cause itching. Rashes associated with secondary syphilis can appear as the chancre is healing or several weeks after the chancre has healed. The characteristic rash of secondary syphilis may appear as rough, red, or reddish brown spots both on the palms of the hands and the bottoms of the feet. However, rashes with a different appearance may occur on other parts of the body, sometimes resembling rashes caused by other diseases. Sometimes rashes associated with secondary syphilis are so faint that they are not noticed. In addition to rashes, symptoms of secondary syphilis may include fever, swollen lymph glands, sore throat, patchy hair loss, headaches, weight loss, muscle aches, and fatigue. The signs and symptoms of secondary syphilis will resolve with or without treatment, but without treatment, the infection will progress to the latent and possibly late stages of disease.
The latent (hidden) stage of syphilis begins when primary and secondary symptoms disappear. Without treatment, the infected person will continue to have syphilis even though there are no signs or symptoms; infection remains in the body. This latent stage can last for years. The late stages of syphilis can develop in about 15% of people who have not been treated for syphilis, and can appear 10 – 20 years after infection was first acquired. In the late stages of syphilis, the disease may subsequently damage the internal organs, including the brain, nerves, eyes, heart, blood vessels, liver, bones, and joints. Signs and symptoms of the late stage of syphilis include difficulty coordinating muscle movements, paralysis, numbness, gradual blindness, and dementia. This damage may be serious enough to cause death.
The syphilis bacterium can infect the baby of a woman during her pregnancy. Depending on how long a pregnant woman has been infected, she may have a high risk of having a stillbirth (a baby born dead) or of giving birth to a baby who dies shortly after birth. An infected baby may be born without signs or symptoms of disease. However, if not treated immediately, the baby may develop serious problems within a few weeks. Untreated babies may become developmentally delayed, have seizures, or die.
Some health care providers can diagnose syphilis by examining material from a chancre (infectious sore) using a special microscope called a dark-field microscope. If syphilis bacteria are present in the sore, they will show up when observed through the microscope.
A blood test is another way to determine whether someone has syphilis. Shortly after infection occurs, the body produces syphilis antibodies that can be detected by an accurate, safe, and inexpensive blood test. A low level of antibodies will likely stay in the blood for months or years even after the disease has been successfully treated. Because untreated syphilis in a pregnant woman can infect and possibly kill her developing baby, every pregnant woman should have a blood test for syphilis.
Genital sores (chancres) caused by syphilis make it easier to transmit and acquire HIV infection sexually. There is an estimated 2- to 5-fold increased risk of acquiring HIV if exposed to that infection when syphilis is present.
Ulcerative STDs that cause sores, ulcers, or breaks in the skin or mucous membranes, such as syphilis, disrupt barriers that provide protection against infections. The genital ulcers caused by syphilis can bleed easily, and when they come into contact with oral and rectal mucosa during sex, increase the infectiousness of and susceptibility to HIV. Having other STDs is also an important predictor for becoming HIV infected because STDs are a marker for behaviors associated with HIV transmission.
Syphilis is easy to cure in its early stages. A single intramuscular injection of penicillin, an antibiotic, will cure a person who has had syphilis for less than a year. Additional doses are needed to treat someone who has had syphilis for longer than a year. For people who are allergic to penicillin, other antibiotics are available to treat syphilis. There are no home remedies or over-the-counter drugs that will cure syphilis. Treatment will kill the syphilis bacterium and prevent further damage, but it will not repair damage already done.
Because effective treatment is available, it is important that persons be screened for syphilis on an on-going basis if their sexual behaviors put them at risk for STDs.
Persons who receive syphilis treatment must abstain from sexual contact with new partners until the syphilis sores are completely healed. Persons with syphilis must notify their sex partners so that they also can be tested and receive treatment if necessary.
